
Snoring and brain outcomes in children
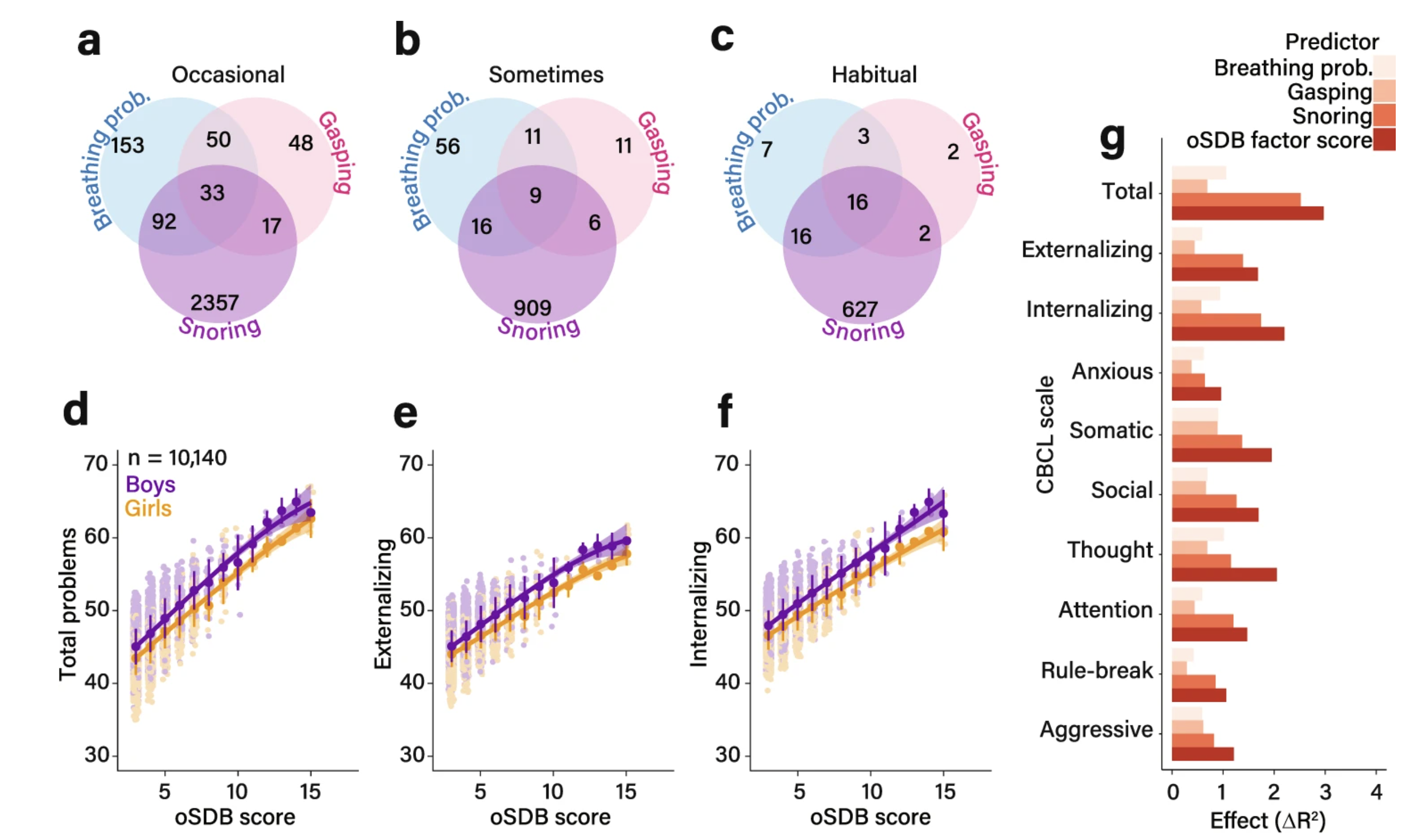
How common are sleep breathing symptoms — and do they affect behavior? Panels a–c show how many of the 10,140 children in this study had parent-reported symptoms of sleep-disordered breathing — snoring, breathing difficulty, and pauses in breathing — and how often. Symptoms were grouped by frequency: occasional (a few times a month), sometimes (once or twice a week), or habitual (more than twice a week). The overlapping circles show children who had more than one symptom at the same time. Panels d–f show that as the overall burden of sleep breathing symptoms increased, children scored higher on measures of behavioral problems — including total, internalizing (e.g., anxiety, withdrawal), and externalizing (e.g., aggression, rule-breaking) problems. This pattern held for both boys and girls. Panel g asks: which symptom matters most for behavior? Among all the symptoms measured, snoring frequency was the strongest predictor of behavioral problems — more so than breathing pauses or nighttime breathing difficulty. These associations remained statistically significant even after accounting for differences in age, sex, race, asthma, and family income.
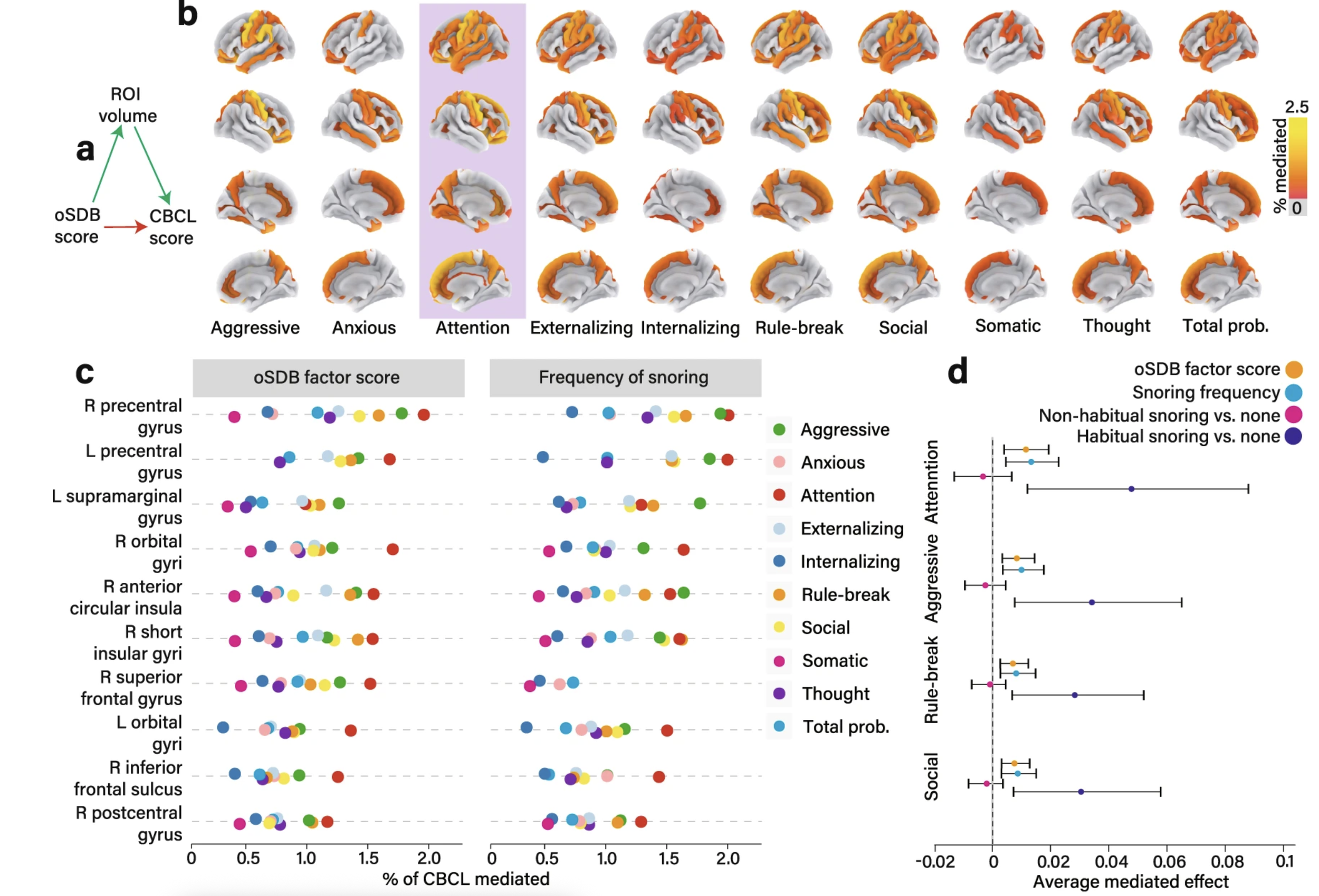
Does brain structure explain the link between sleep breathing problems and behavior? Panel a outlines the core question: can the relationship between sleep-disordered breathing and behavioral problems be explained — at least in part — by differences in brain structure? To test this, the researchers used a statistical approach called mediation analysis, which estimates how much of the connection between two things (here, sleep symptoms and behavior scores) is "carried through" a third factor (here, the volume of specific brain regions). Panel b maps these results onto the brain's surface. Regions where smaller cortical volume accounted for a meaningful portion of the sleep–behavior relationship are highlighted. Attention problems showed the most widespread and strongest effects, meaning that frontal lobe volume loss appeared most relevant to children's difficulties with focus and self-regulation. Panel c shows the top ten brain regions driving these effects. Importantly, the results looked nearly identical whether researchers used the overall sleep symptom burden or snoring frequency alone — reinforcing snoring as a reliable and clinically practical indicator. Panel d addresses a practical question: how much snoring is too much? When children were divided into non-snorers, occasional snorers (fewer than three nights a week), and habitual snorers (three or more nights a week), the brain-mediated behavioral effects appeared only in the habitual snoring group. Occasional snorers were statistically indistinguishable from children who didn't snore at all. This finding directly supports the clinical threshold already used by pediatricians to decide when snoring warrants further evaluation.