
Behavioral Outcomes of Adenotonsillectomy
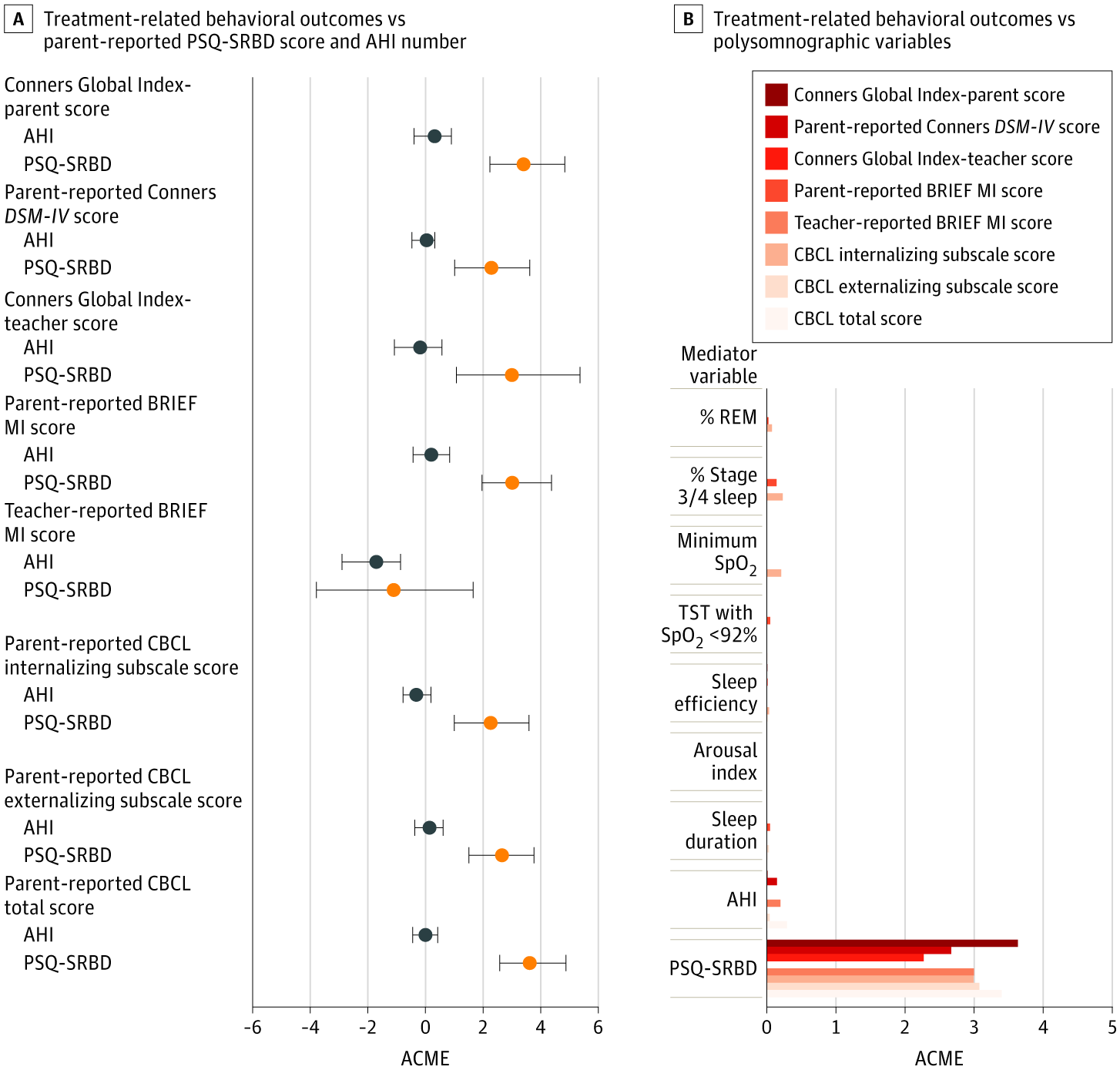
What drives behavioral improvement after treatment — airway obstruction severity or symptom burden? This figure uses mediation analysis to ask a specific question: when children's behavior improves after treatment for sleep-disordered breathing, what is actually responsible for that improvement? Two candidates are tested — the severity of airway obstruction measured objectively by sleep study (AHI, the number of breathing pauses per hour), and the overall burden of sleep breathing symptoms reported by parents (PSQ-SRBD score). Panel A compares these two candidates head to head across eight behavioral outcome measures spanning attention, executive function, and behavioral problems. The horizontal bars show the average causal mediation effect (ACME) — essentially, how much of the treatment benefit can be attributed to each variable. Across every behavioral outcome tested, parent-reported symptom burden (orange) consistently showed a larger mediation effect than the objective AHI (gray). In other words, the degree to which parents perceived their child's breathing symptoms improved after treatment was a stronger driver of behavioral gains than the raw count of breathing pauses on the sleep study. Notably, the Teacher-reported BRIEF score was the one measure where both AHI and PSQ-SRBD pointed in the negative direction, suggesting a more complex relationship for teacher-observed executive function. Panel B broadens the comparison to include all variables measured on the sleep study — including sleep stages, oxygen levels, sleep efficiency, arousal frequency, and sleep duration — alongside AHI and PSQ-SRBD. The results are striking: PSQ-SRBD was by far the strongest mediator of behavioral improvement across all outcomes, with bars extending well beyond every polysomnographic variable. AHI showed a small but visible effect, while measures such as oxygen levels, sleep efficiency, arousal index, and sleep duration contributed minimally to behavioral change. Taken together, the figure suggests that how symptomatic a child appears to their parents — not how severe their sleep study looks — is the more powerful predictor of whether behavior will improve after treatment.
Cognitive and Behavioral Outcomes of SDB
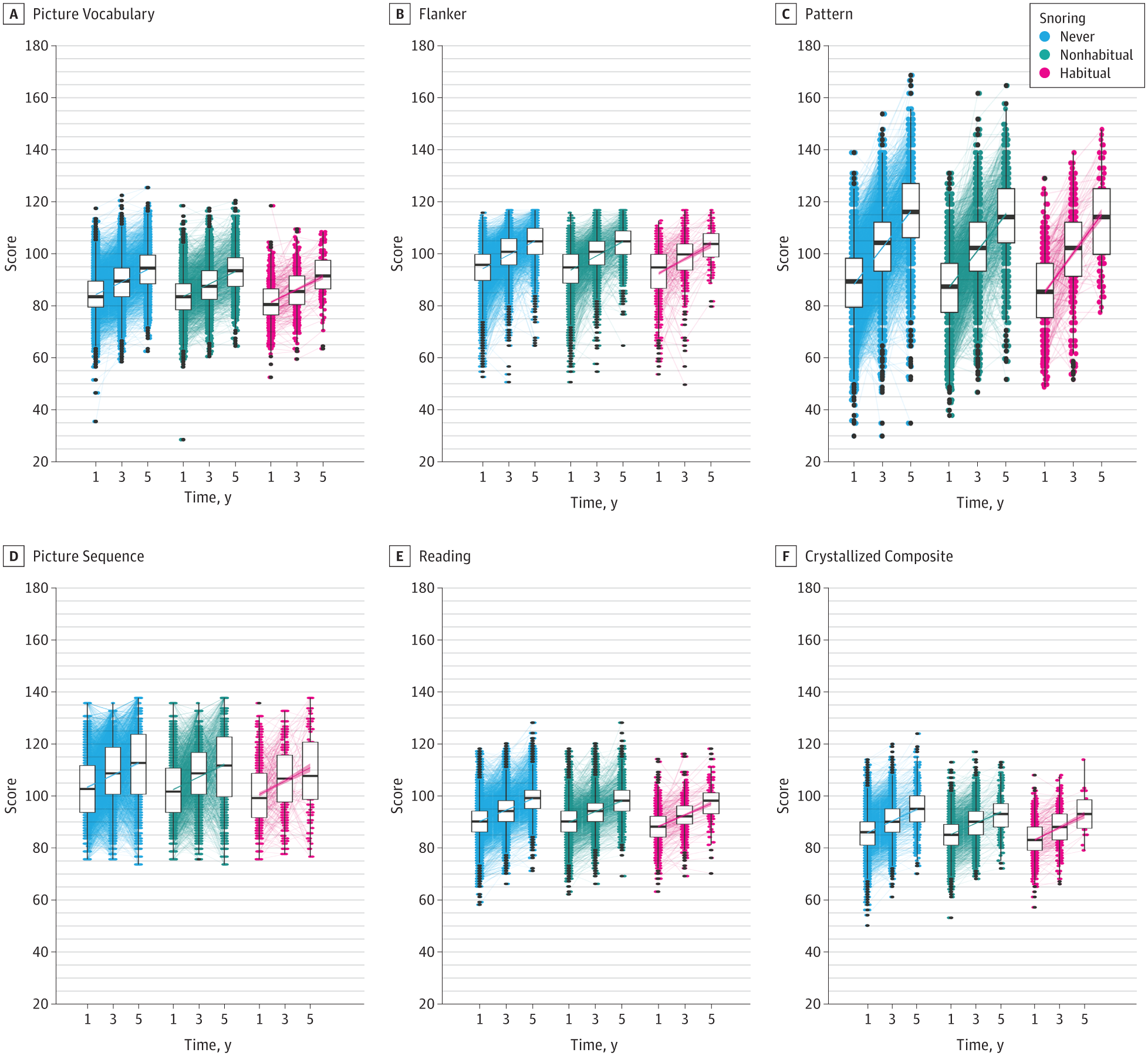
Do children who snore score lower on cognitive tests — and does this change over time?This figure tracks cognitive performance across six domains from the NIH Toolbox — a standardized battery of tests covering areas such as memory, attention, processing speed, and language — at multiple time points, grouped by how often children snore. Children are divided into three groups: those who never snore (blue), those who snore occasionally but not habitually (green), and those who snore habitually — meaning three or more nights per week (pink). For each group and time point, the box plots show the spread of scores: the middle line is the median, the box edges mark the range where the middle half of children fall, and the extending lines capture the full spread of typical values. Black dots are outliers. The connecting lines with shaded confidence intervals trace how each group's scores change across time, making it possible to see not just whether snorers score differently at any single point, but whether the gap between groups widens, narrows, or persists as children grow. The key question the figure addresses is whether habitual snoring is associated with a meaningful and consistent cognitive disadvantage — and whether that disadvantage is stable, worsening, or potentially reversible over the course of the study.